Original list of terms by Jerri Jenista, MD; some drug definitions from Karen Hauff, Pharm.D; updates and intro by Julian Davies, MD
Big thanks to the original authors for their gracious permission to adapt and publish this list, for the pioneering work of Dr Jenista and the staff of the International Adoption Center, and the counsel of our colleagues in Russia and on the Adoptmed listserv of adoption medical professionals.
It should be noted that we are not Russian doctors, nor were we trained in the mysterious art of Russian neurology, so take this for what it is: a glossary of medical terms found in Russian (and Ukrainian, and Kazakh, and other former Soviet Union) medical charts based on the interpretations we've collected over the years. Other definitions for many of these terms exist, they are not always used consistently (or translated accurately), and the degree of concern over these diagnoses will vary based on other factors in a child's history.
We would urge you to discuss the specifics of a particular referral with an international adoption specialist who can incorporate these medical terms into the context of a child's growth, development, physical features, and signs of more familiar Western medical conditions.
Why so many neurologic diagnoses in Eastern European referrals? Some possible reasons:
Russian medicine tends to list issues that we might consider "risk factors" or "things to watch for" as diagnoses (thus, lack of prenatal care can become "risk for intrauterine infection")
many diagnoses are provided by specialists and hospitalists, notoriously the neurologists, many of whom seem to have "favorite diagnoses", and incentives to overdiagnose in general
a persistent Soviet-era pessimism about the birth process; even with a (to us) healthy delivery they are quite worried about interruptions of blood and oxygen to the baby's brain, kinking of the spinal cord, and so on ... their descriptions of the birth process (and occasional interpretations of newborn spinal xrays) can leave one marvelling that babies are born with their heads still attached
a tendency to interpret what to us are normal, immature newborn behaviors (startle reflex, trembling chin, mottled skin, belching, etc) as signs of neurologic damage
and a subsequent tendency to ascribe what we might call normal infant maturation to recovery from neurologic illness, thanks to massage, medications, supplements, and other typical treatments
when it comes to orphanage-raised children (who, admittedly, do come from higher-risk backgrounds), there may be a bit of cultural pessimism about outcomes
Or, on the 'flip' side:
"Sometimes they diagnose just to show they care ..."
"It's all just a big jobs program for Russian neurologists."
"This diagnosis, in Western terminology, means that the child was born in Russia."
"It's the 'shotgun' approach to diagnosis - if you label all the children with neurologic impairments, you can rest easy that you haven't missed any of the actual diagnoses."
An article just published in Lancet sheds some light on the practice of pediatrics in Russia, Kazakhstan, and Moldova in a systematic review of hospitals. Essentially, the pediatricians are found to be dedicated and proud of their work, but hampered by antiquated, unproven protocols that over-diagnose, over-test, and over-medicate young children, not to mention the outdated or missing diagnostic equipment and treatment supplies. Kids languish in hospitals far too long for minor illnesses, and in the case of orphans, typically receive very little stimulation (we've found that children often do worse in hospitals than orphanages). Children are routinely prescribed "large numbers of ineffective or dubiously effective treatments" (avg of 5 at a time in Kazakhstan) for vague indications, without adequate monitoring of potentially dangerous side effects.
Medical anthropology aside, orphanage doctors naturally have a good deal of experience with orphanage-raised children, and it can be very helpful to seek their opinion on how a child is doing. Sometimes they are stuck with diagnoses from other medical settings (see above) that they are not as concerned about, or can provide useful information on trends over time.
A brief note on cerebral palsy: It's remarkable how much time we spending talking and thinking about and trying to rule out CP in Russian referrals ... when in fact we haven't had more than a few Russian (and Kazakh and Ukrainian) children that arrived here in the past few years that turned out to have significant CP.
Not that we're going to stop asking followup questions about muscle tone trends, and rate of development, and if there are current concrete neurologic concerns, or flat-out "does this child have CP?" ... but I think it probably deserves much less anxiety than it gets. The Russian docs seem to do a good job recognizing cerebral palsy, or we do, or it's just not that common, compared to orphanage-related delays, transient dystonia (periods of higher or lower muscle tone in infancy that resolve), low tone and strength from lack of stimulation or mild rickets, and other issues that get better with time, stimulation, and nutrition.
Not that we don't see kids with neurologic and developmental issues ... but we see a lot more language delay, poor motor planning, sensory issues, fetal alcohol spectrum concerns, insecure attachments, learning problems, ADHD, etc than we do cerebral palsy. And CP can certainly be a milder disability than some of the above.
On that note, without further ado ... here it is, the evolving glossary of Eastern European medical terms and treatments:
Abnormal chordae (trabeculae): Extra muscle tissue in the wall of the heart, usually the left ventricle (lower chamber). Typically found by routine echocardiogram of the heart. This is an "incidental finding" - it does not cause symptoms or disease.
Abominum: Antispasmodic used in the treatment of gastritis and colitis.
Abstinence syndrome: Newborn withdrawal syndrome (or NAS), usually from narcotics.
Actovegin: Calf's blood extract used by Russian doctors and Tour de France cyclists to improve oxygen-carrying capacity.
Adiposogenital syndrome: Freohlich's syndrome, i.e., truncal obesity with hypogonadism and short stature in boys. Sometimes used (incorrectly) to describe obese boys with delayed sexual maturation.
Alcoholic fetopathy: Fetal alcohol syndrome.
Alienist: Psychiatrist.
Alimentary subnanism: Short stature due to malnutrition, illness or other medical problems past the first year of life. Also called hypostatura in younger children.
Alpha tirroxinum: Thyrotropinum, thyrotropin or TSH.
Aminalon (gamma aminobutyric acid): An antihypertensive medication to decrease pressure in the brain.
Ampiox: Antibiotic combination of ampicillin and oxacillin.
Anamnesis: Medical history.
Ankyloglossia: Tongue-tied.
ARVI: Acute respiratory viral illness (a "cold").
Asparkam: Potassium-magnesium combination used for cardiac arrhythmia.
ATP: Adenosine triphosphate, a coenzyme to improve muscle contraction.
Australia antigen: Also written as HbsAg. Hepatitis B surface antigen, marker for current infection.
Baclofen (Baclon): Drug used to treat spasticity such as that seen with cerebral palsy or spinal cord trauma.
Baktysutil (?): see Orobicin
Bendazol (dibasol or tiabendazole): A vasodilator.
Bilary dyskinesia: Functional problem with the motility of the biliary tract, often (over)diagnosed from ultrasound examinations.
BL: Test for the causative bacterium of diphtheria.
Brulamycin (tobramycin): Aminoglycoside antibiotic.
Calcium orotate (calcium salt of orotic acid): Used in the treatment of hyperuricemia and hypercholesterolemia; also used to treat liver disorders.
Cardiopathy: Any functional condition of the heart, e.g., rapid or slow or irregular heartbeat, heart murmur, poor heart function. Often transient and nonspecific.
Catarrhal otitis: Middle ear inflammation (redness only) without pus, accompanied by an upper respiratory tract infection. The condition American pediatricians call otitis media (redness of the ear drum with pus) is called "purulent otitis."
Cavinton (vinpocetine): Used to treat cerebrovascular and cognitive disorders.
Cefamezin (cefazolin): First-generation cephalosporin antibiotic.
Cefamid (cephradine): Semisynthetic cephalosporin antibiotic.
Cerebro-asthenic syndrome: Same as neurasthenic syndrome.
Cerebrolysin: Porcine brain extract used to treat nervous system disorders.
Cinnarizine (Sturgeron, Midronal): An antihistamine drug used to control vomiting by decreasing pressure in the brain, also to selectively dilate brain blood vessels.
Citral solution, citric acid solution: Used to relieve flatulence and pain; ingredient found in herbal remedies used for a variety of disorders.
COE: ESR - erythrocyte sedimentation rate (a marker for inflammation of infection).
Colpitis: Inflammation of the cervix or vagina.
Corvalol: Phenobarbital-containing OTC medication.
Complamin (xanthinol nicotinate): Used to treat hypercholesterolemia, peripheral arterial disorders; cerebral circulatory and metabolic disorders; retinal vascular disorders; Ménière’s disease and hearing disorders.
Coprogram: Stool examination.
D=S: Dexter=Sinister, that is, the right equals the left. Usually referring to muscle tone or reflexes in the extremities.
Diamox (diacarb, fonurit, acetazolamide): Diuretic drug (carbonic anhydrase inhibitor) used to decrease pressure in the brain, sometimes to help control seizures.
Diaphanosopy: Examination of any body part by transillumination (shining a light through or against it).
Dibasol (bendazol): Vasodilating drug.
Dropsy of the testicles: One of my favorite "lost in translation" diagnoses. It means hydrocele, which is a benign fluid collection in the scrotum that resolves with time.
Dysbacteriosis: Loose or diarrheal stool following lack of breast-feeding, illness or a course of antibiotics. Due to changes in the normal bacterial flora of the intestine. Treated first with an antibiotic to decontaminate the gastrointestinal tract and then with "ferments and enzymes," similar to our treatment with lactase (milk sugar enzyme) or probiotics (live cultures found in yogurt).
Dysmetabolic nephropathy: Secondary impairment of kidney function following a insult such as malnutrition. There is no structural damage to the kidney. Most cases are reversible once the underlying disease is taken care of.
Electrophoresis: Method of giving medication. Substance is applied to the skin, usually over the affected part, and then a mild electric current is run through is.
Encephabol (pyritinol): Used to treat rheumatoid arthritis, cerebral insufficiency, organic brain disorders, migraine and trigeminal neuralgia.
Epicrisis: The word means "time period." It is used in two different ways.
*When a patient is admitted to the hospital. Written summaries of the condition and progress are made at admission, at about 10 days and at discharge. These are referred to as epicrisis.
*Developmental progress is codified by the skills which are typically achieved in a certain time period or epicrisis. In the first year of life there are well child check-ups at 1, 2, 3, 6, 9 and 12 months of age. Each visit encompasses an epicrisis from the previous point. As the child gets older, the epicrisis periods are longer usually 6-month intervals. Thus a 9 month old who is "delayed 1 epicrisis" has the expected development of a 6 month old.
Euphyllin (aminophylline): Bronchodilator, for wheezing or asthma.
Exudative diathesis: Skin rash usually attributed to feeding problem, especially food allergy, or a drug reaction. The skin is usually red and dry; the child may scratch until it oozes or bleeds. If the rash persists for months or is very severe, it may be considered eczema.
Ferrimed (vitamin B substances, iron polymaltose, folic acid): Used in the treatment of iron-deficiency anemia.
Furagin (furazidin): An anti-infective agent.
Furanthril or Furantral (furosemide): Loop diuretic.
Gestosis: Morning sickness. Sometimes the term is used (incorrectly) to refer to toxemia or pre-eclampsia manifest in the mother during pregnancy by protein in the urine, edema (swelling), high blood pressure and, rarely, other neurologic problems.
Glutamic acid: A dietary supplement.
Grefe symptom: "Sundowning" of the eyes (sclera is visible above the iris when the eye is open but relaxed) sometimes indicating hydrocephalus.
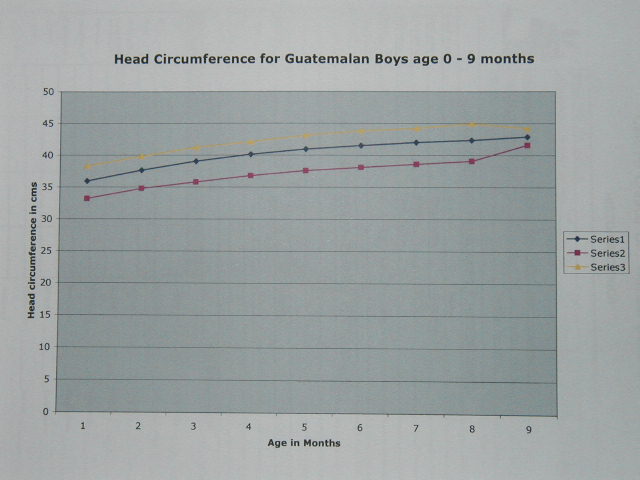
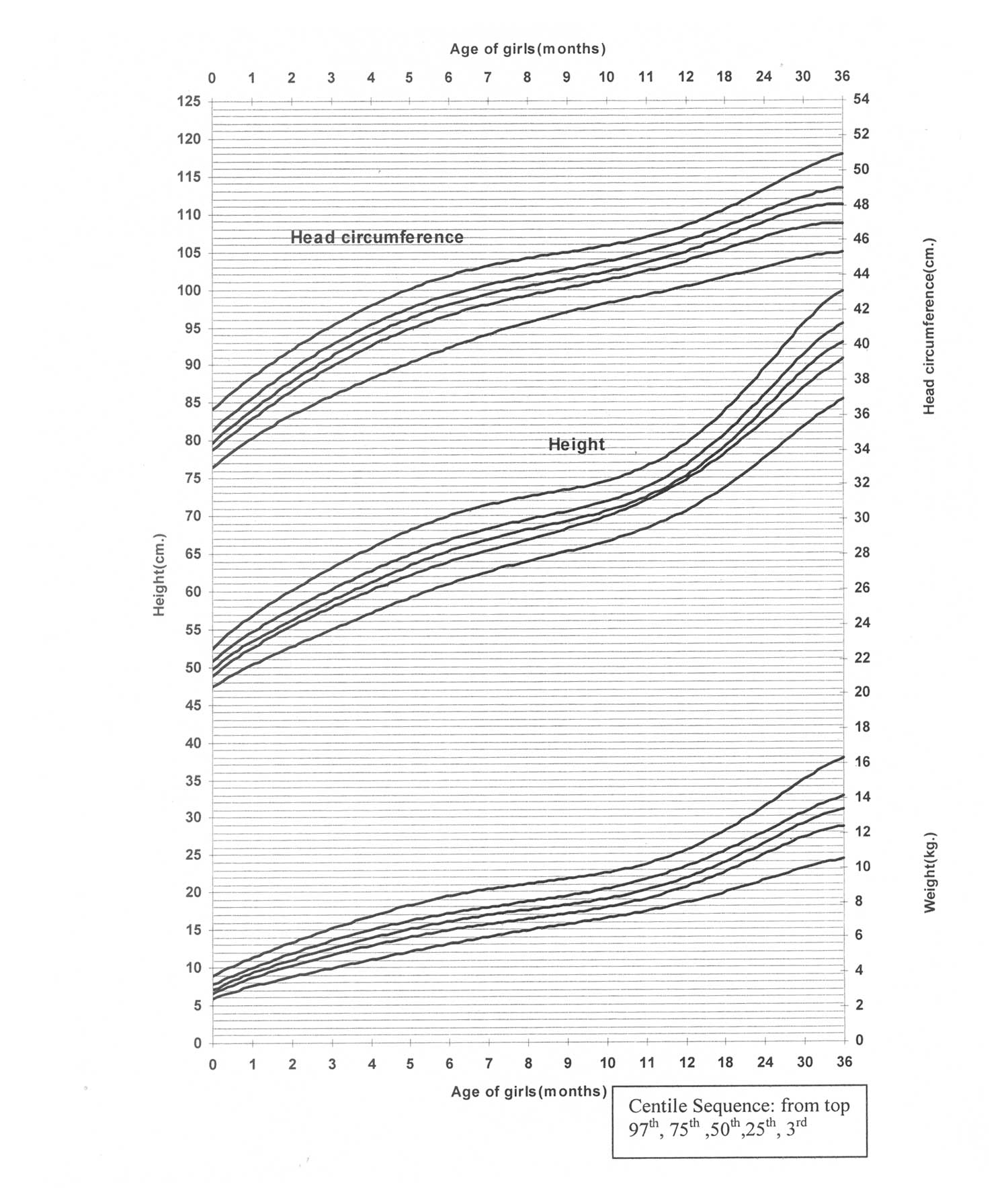
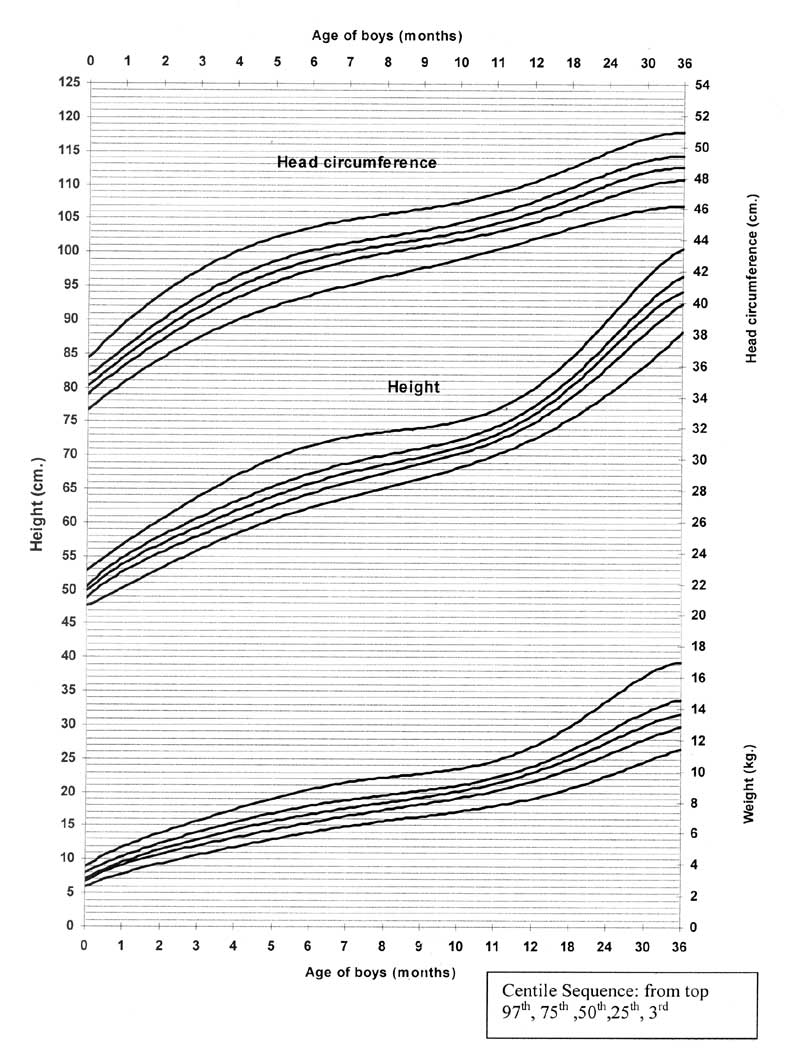
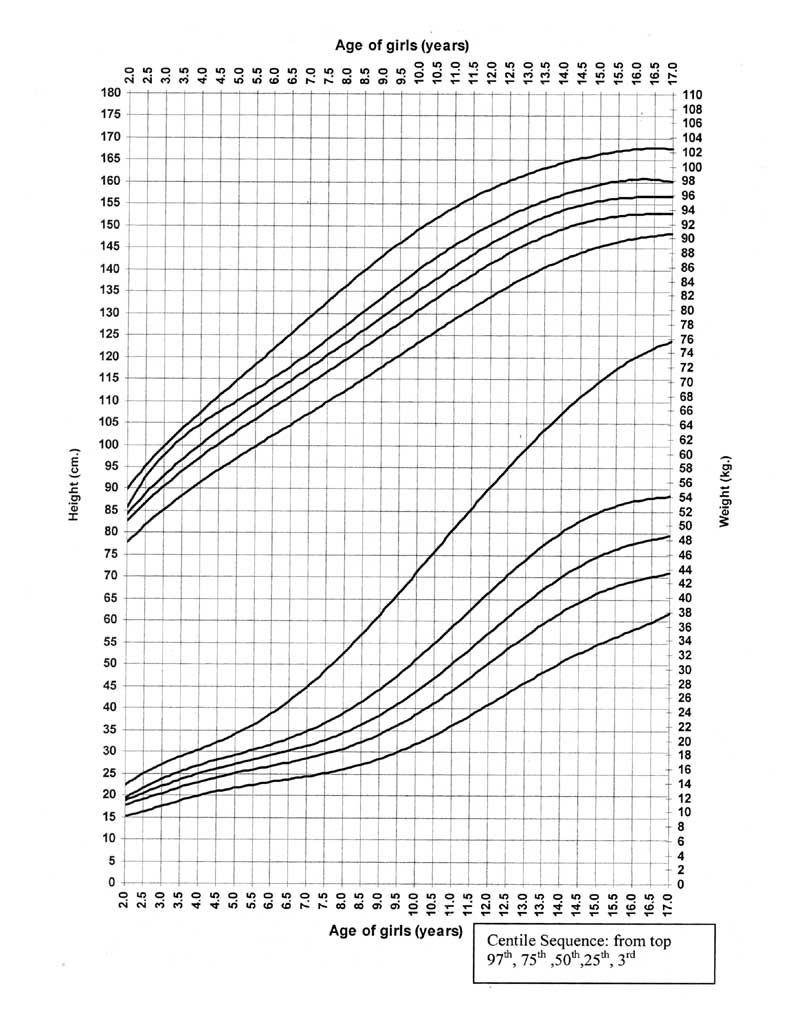
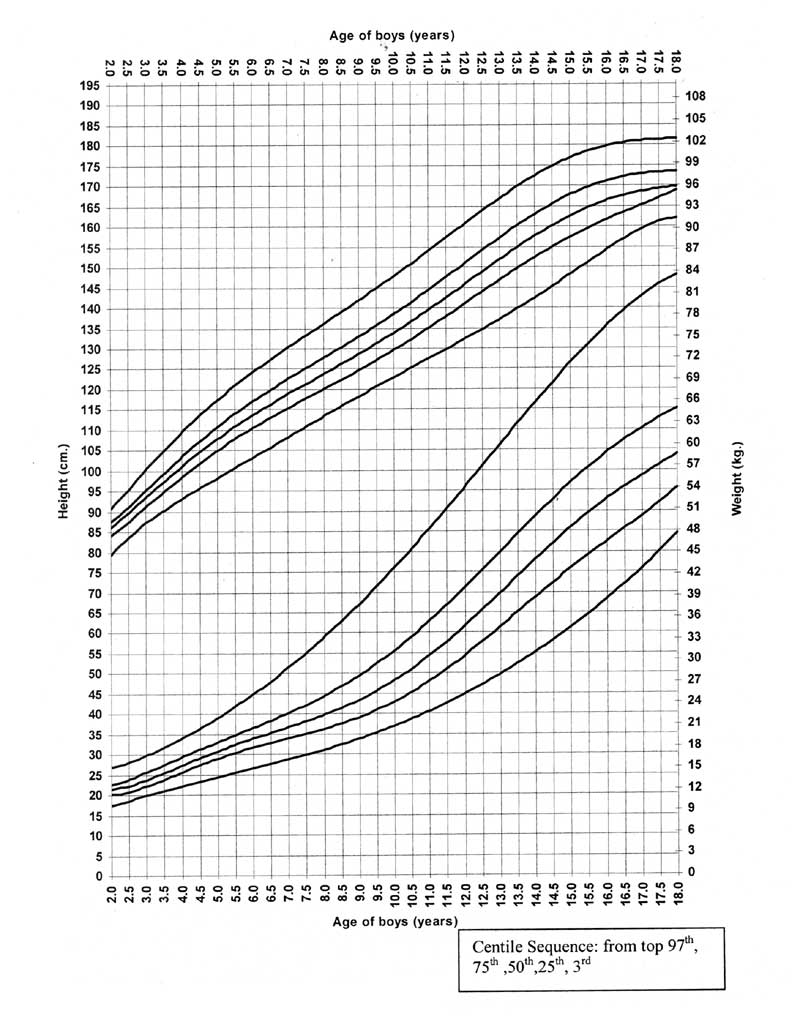
Growth: Classified by percentile as on North American growth charts. Average or normal growth is considered to be between the 25th and 75th percentiles for age and sex. Growth patterns:
Harmonic: Height, weight and chest circumference are all at or near the same percentile.
Dismarmonic: One of height, weight or chest circumference is markedly different in percentile from the other parameters.
Mesosomatic: Height, weight and chest circumference are all average.
Microsomatic: Height, weight and chest circumference are all low.
Macrosomatic: Height, weight and chest circumference are all high.
Gypotrophy: Same as hypotrophy.
Health group : Classification of children's health condition. Groups I-III are considered basically healthy children, although treatment may be necessary. Sometimes an A or B is appended; certain diseases belong to these A or B subgroups. These health groups are pretty vague and inconsistent, in our experience.
Group I: Absolutely healthy (unusual to see on orphans records or any records, for that matter)
Group II: Minor problems such as enlarged tonsils or a mild chronic condition such as gastritis with no symptoms.
Group III: A chronic condition with frequent exacerbation, for example, asthma under poor control.
Group IV: Severe health condition with some degree of disability.
Group V: Physical handicap such as a missing extremity
Hyalase, Wydase (hyaluronidase): Adjuvant to increase the absorption and dispersion of other injected drugs or for hypodermoclysis.
Hyperexcitability (neuroexcitablity, neuro-reflex irritability) syndrome: Similar to muscular dystonia but diagnosed within the first 3 months of life. Noted when the infant has marked reactions to stimuli (such as being moved or disturbed), especially if tremor, increased newborn reflexes, trembling chin or frequent belching is present. It may result in "movement disorder" at an older age.
Hypermetropia: Far-sighted.
Hypertension syndrome: Same as hypertension-hydrocephalic syndrome.
Hypertension-hydrocephalic syndrome: Clinical diagnosis based on one or more criteria alone or in combination:
Seizures
Increased muscle tone
Brisk reflexes
Firm or tense fontanel (soft spot)
Pulsation of the fontanel Tremor
Jitteriness
Large head circumference
Dilated blood vessels over the scalp
Prominent or bulging eyes
"Sundowning" of the eyes
Bluish discoloration over the bridge of the nose.
May be "confirmed" by ultrasound of the brain looking for dilation of the ventricles (fluid-filled spaces in the brain) or changes in the blood flow pattern. Considered in most children to be a transient condition secondary to the birth process. Treated with certain vitamins, diuretics, and/or other drugs to improve blood flow to the brain. Surgical shunting is very rare. It is not equivalent to the Western term "obstructive hydrocephalus".
The condition is considered to be "subcompensated" when the child still has some minor signs or symptoms but is doing okay. It is "compensated" when there are no clinical signs except perhaps for a head slightly out of proportion with the rest of the body: at this point, the child expected to be normal.
Hypometropia: Myopia, near-sighted.
Hypostatura: Short stature due to malnutrition, illness or other medical problems. Past the first year of life, it is called alimentary subnanism.
Hypothyrosis: Hypothyroidism, treated with oral thyroid replacement. Screening for hypothyroidism is usually carried out at the first well-child check-up at one month of age.
Hypoplasia: Short stature with no other problems, usually genetic or "constitutional". Also used to refer to under-development of any organ such as a limb, the testis, an eye, etc.
Hypotrophy: Weight lower than expected for age. May be further described as mesosomatic or microsomatic, harmonious or disharmonious, depending on changes from previous growth and the relationship to the height and chest circumference.
Hypoxia of the newborn: Lack of oxygen at or before delivery, usually diagnosed if it was a difficult pregnancy, labor or delivery, if the baby needed a lot of resuscitation at birth or if specific abnormalities are noted in the placenta (afterbirth). When severe oxygen deprivation was felt to occur, the word "asphyxia" is used, although this seems to have a loose definition over there. "Prenatal hypoxia"" is a vague term, sometimes used with the wording "non-specific intrauterine infection" to explain away low weight or asymmetric reflexes or tone in a full-term baby.
Hypoxic (metabolic) cardiopathy: A clinical diagnosis, sometimes confirmed by "metabolic changes in the EKG." This refers to any number of mild changes in circulation such as perioral cyanosis (blueness around the lips and nose), irregular heartbeat, mottled skin, anemia or rickets. This is a transient condition, which resolves when the underlying condition is treated. Term may be also used for more serious conditions such as myocarditis.
Increased seizure readiness syndrome: When a child has an evaluation for suspected seizures or some other problem, an EEG of the brain may be done. The term is used to describe the finding of an abnormal focus on the EEG or when a child has increased muscle tone not related to cerebral palsy. Usually no treatment is given.
Intrauterine pneumonia: Applied broadly when a newborn has respiratory distress or "rule-out sepsis" (signs of infection).
Ischemia of the newborn: Usually referring to lack of blood flow to the brain, used in the same way or as a synonym to "hypoxia of the newborn."
Lambliosis (lambliasis): Giardia infection.
Lidaza: A very popular enzyme drug, bovine hialuronidase extracted from testicles. Given by injection or electrophoresis to decrease scarring form chronic inflammation, for example, after abdominal surgery.
Limonal: Light magnesium carbonate used to treat constipation.
Little's disease: Cerebral palsy.
Logopedist: Speech therapist.
Lues, Luis: Syphilis.
Luminal (phenobarbital): An anticonvulsant, unfortunately used in many children who do not have epilepsy.
Midronal: Same as cinnarizine.
Minimal brain dysfunction: Used variably to describe transient neurology signs such as hyperactivity or short attention span, or as a followup diagnosis to "perinatal encephalopathy".
Mixed genesis: A health condition with more than one contributing or underlying causes.
Movement (motor) disorder: This is one result of delayed motor skills. For example, a 10 month old who cannot crawl has a movement disorder. This is not considered a serious diagnosis in contrast to more pronounced forms, like spastic tetraparesis. It is sometimes used when a child is not "perfect" but no other diagnosis can be made.
Mucoviscidosis: Cystic fibrosis.
Muscular dystonia: Muscle tone is considered to be dependent on the emotional condition of the baby. A normal child should be calm with appropriate relaxed tone. Muscular dystonia is present when the tone is very high (jittery or irritable) or is labile (changes rapidly). This is not a permanent condition but changes over brief time periods (an hour) as the baby's state changes (from sleepy to alert, etc.)
Myodocalm (tolperisone or mydeton): Centrally acting muscle relaxant.
Myotonic syndrome: Vague terminology used to describe changes in muscle tone, especially low tone (hypotonia).
Narcomania: Drug addiction.
Natal trauma of the spinal cord: Diagnosis made at the time of delivery based on the process of the delivery itself and the state of the newborn. Risk of this condition is considered to be present if the delivery was difficult, i.e. the baby had to be rotated, the head turned, etc. or if the baby has certain signs such as abnormal tone, tremor, irritability, mottled discoloration of the skin, pallor or sweating. This is a functional condition; that is, it will resolve with treatment (massage, application of mild electrical current to the skin over the affected part, etc.) Even when the condition has resolved, the diagnosis is often kept until the age of 1 year. It is frequently used as a contraindication to giving immunizations, with the thought that vaccinations may exhaust the immune system and prevent complete resolution of the spinal trauma. May be accompanied by xray "findings" of "subluxation of C1-C3 vertebrae." Scarier-sounding than it typically turns out.
Nephropathy: Generalized term used to describe any past or present abnormality in kidney function, usually used for conditions thought to be transient.
Neurasthenic syndrome: Condition when a child gets tired very easily or irritated for little or no reason. Manifests in many ways, e.g., irregular or fast heart beat, poor sleeping habits, becoming very red or very pale with vegetative functions (feeding, burping, passing stool) in infants.
Nicospan (nicotinic acid): B-complex vitamin.
Nootropyl (nootrops, piracetam): Drugs used to treat strokes, vertigo, learning disability and other brain disorders. Occasionally used in Down's Syndrome and sometimes in difficult births.
Obstructive bronchitis: A viral respiratory infection with wheezing. This can be wheezing from the inflammation and airway mucous of viral bronchiolitis, or a wheezing tendency that may evolve into asthma. Roughly speakly, 1/3 of infants and toddlers who wheeze for the 1st time won't wheeze again, 1/3 will have wheezing with colds and such but outgrow it by school-age, and 1/3 will continue to have asthma symptoms into later childhood and beyond.
Oligophrenia: Functional mental impairment, meaning the person is not operating at the expected level, usually not diagnosed until older than 4 years. Vague and frustrating "diagnosis" for us, that may be caused by any number of inheritable or environmental influences such as genetic syndromes, learning disabilities or mental retardation of unknown cause, fetal alcohol spectrum issues, head trauma, infection, orphanage care, social chaos, poor schooling, and other adverse experiences, etc ...
Could refer to an adult that would be cognitively "normal" if tested but has had a hard-knock life and is seeking disability pension, or an orphan unfairly labeled as "debil" by a cursory examination at 3-4yo, or a person with mild mental delay, or severe mental retardation. Not unusual to hear that a birth parent has this label, very hard to know whether this is an inheritable condition in any given case. It does not refer to schizophrenia, although it is useful to ask about mental health concerns. Nor does it refer to a rock opera by the Who.
Onanism: Masturbation.
Open oval window: Patent foramen ovale, the normal embryological connection between the two upper chambers (atria) of the heart, typically detected on routine newborn heart ultrasound. Is not considered a heart defect, and usually closes on its own. Not the same as an atrial septal defect (ASD).
Panagin (aspartic acid): A dietary supplement.
Panangin: Hungarian-made equivalent of Asparkam.
Pancreatin: Pancreatic enzymes with protease, amylase and lipase activity used to treat pancreatic insufficiency associated with CF and pancreatitis.
Pantogen (calcium pantothenate): A component of coenzyme A which is essential for the metabolism of carbohydrate, fat and protein; B complex vitamin.
Pantogar (calcium pantothenate; thiamin nitrate; medicinal yeast; cystine; keratin; aminobenzoic acid): Used to treat disorders of the hair and nails.
Pantotene: Vitamin B5.
Papaverine: Synthetic analog of an antispasmodic substance found in the opium poppy. Used to relax involuntary muscles (blood vessels, intestine, etc.)
Pentagin: Pentazocine, narcotic analgesic.
Perinatal (prenatal) encephalopathy : Variably translated as "perinatal lesion or affectation of the central nervous system," "encephalopathia," and many others. One or more risk factors present in the history of the mother or the baby, which may allow, or not, for a poor neurological outcome (see table that follows). Some variation of this on >90% of Russian referrals, thus has very little, if any, predictive value for any particular child. Best to look for more concrete information in the referral.
Maternal Factors
Lack of known medical history
Drug, alcohol or cigarette use
No prenatal care
Anemia
Past miscarriages, abortions or premature deliveries
Young or old maternal age
High number pregnancy
Chronic health problems
Infections
Poor social situation
Difficult or complicated delivery
Abnormal placenta
And many others
Infant Factors
Low Apgar scores
Abnormal muscle tone or reflexes
Jaundice
Seizures
Irritability or depression
Tremor
Poor suck, feeding problems
Abnormal ultrasound of brain or other parts of body
Intrauterine or perinatal infections
Prematurity
Abnormal prenatal growth
Abnormal laboratory tests
And many others
Perinatal trauma (affectation) of the CNS (central nervous system): Synonym for perinatal encephalopathy. Also called perinatal lesion, cranio-cerebral trauma of the newborn and other variations.
Phthisiologist: Specialist in the management of tuberculosis.
Piloecstacy of the kidneys: Dilatation of the collecting system just next to the kidneys, considered to be "pre-hydronephrosis."
Piracetam: see Nootropyl
Positive dynamics: Continuous improvement or in the recovery phase in any condition, but especially in growth and development. A child with positive dynamics is expected to be normal.
Prematurity: Determined by maternal history, birth weight, and/or a scoring system such as the Dubowitz (same as used in North America). Described as stage or degree (terms not used in US), see table below.
Stage or Degree
Gestational Age
Weight
1
36-37 weeks
2001-2500 grams
2
32-35 weeks
1501-2000 grams
3
28-31 weeks
1000-1500 grams
4
<28 weeks
<1000 grams
Psycho-affective respiratory attack: Breath-holding spells.
Pyramidal insufficiency: Infant considered to be at risk of cerebral palsy because of adverse perinatal history (e.g., extreme prematurity or low birth weight) and/or because of abnormal physical examination (e.g., increased tone or reflexes, asymmetry of reflexes, delayed development). Usually cannot be confirmed as cerebral palsy until after 12 months of age as most children will improve before then. Usually is apparent by 6 months of age and, if it is going to resolve, disappears by 1 year. This is a commonly encountered diagnosis.
Pyridoxine (pyridoxal phosphate): Vitamin B6, often used with other B vitamins to treat brain disorders.
Rachitis: Rickets, bone disease due to lack of vitamin D (see table below).
Stage or Degree
Time to develop
Clinical signs
1
Weeks
Minimal or nothing at all.
2
2-3 months
Delayed development due to bone pain and weakness.
3
Many months
Marked developmental delay, bone deformation (bowed legs), abnormal skull shape or size (boxy forehead), poor muscle tone and strength.
Relanium (diazepam): Long-acting benzodiazepine used as a sedative, anxiolytic and anticonvulsant.
Retrobolin (nandrolone): Anabolic agent.
RIF: "Immuno-fermentation reaction" - a test for syphilis.
RIT (or RIBT): "Immobilization Treponema Pallidum Reaction" - another syphilis test.
Rudotel (medazepam): Long-acting benzodiazepine with uses similar to diazepam, such as anxiolytic, sedative, anticonvulsant, etc.
Sana-Sol: Multivitamin and mineral supplement.
Seduxen (diazepam): Long-acting benzodiazepine used as a sedative, anxiolytic and anticonvulsant.
Sexual crisis: Bloody discharge from the vagina of the newborn or breast swelling, with or without milk discharge. Normal finding, noted in the first two weeks of life, due to withdrawal of maternal hormones.
Sonne Dysentery: Lower intestinal infection with Shigella bacteria, causing loose/watery to bloody/mucoid stools, occasional neurologic symptoms like seizures and lethargy, treated with antibiotics and fluids.
Spastic tetraparesis: This is a potentially more serious form of movement disorder in children less than 12 months of age, graded from mild to severe, involving all 4 limbs. In the worst case, the child barely moves at all. If treatment (massage and physical therapy) is started early, this is usually easily correctable but some children have persistent neurological findings. When we see this diagnosis, we make sure to ask about trends of muscle tone and development over time, and if the child is felt to be showing signs of cerebral palsy.
Specialized Schools: Courtesy of Dr Gordina, here's a list of Russian specialized ("correctional") schools:
Type 2 - For children with hearing problems
Type 3 - For children with significant vision problems (legally blind)
Type 4 - For children with poor vision
Type 5 - For children with significant speech/language delays
Type 6 - For children with motor and orthopedic problems (mostly CP)
Type 7 - For developmentally delayed children
Type 8 - For children with intellectual disabilities (mental retardation)
Squint: Crossed eye.
Stage of condition: The progression of a disease:
Recuperation or rehabilitation - Improving but still requiring treatment.
Subcompensated - Abnormal, clinically unstable may deteriorate.
Compensated - Abnormal but stable.
Recovery - Condition or illness completely resolved.
Stigma: Any one or more minor congenital abnormalities such as low set or posteriorly rotated ears, high arched palate, epicanthal folds, broad thumb, etc... When no particular syndrome is identified, North American physicians sometimes refer to such as child as a "funny looking kid," or to use a more technical term, "mildly dysmorphic". A child with 3 or more minor congenital anomalies is at increased risk for a broader syndrome.
Stomatologist: Dentist.
Sugeron: Same as cinnarizine.
Sumamed: Azthromycin (Zithromax), a macrolide antibiotic.
Thymomegaly: Enlarged thymus, "diagnosed" from the normal thymic shabow on infant xrays, and of no clinical significance.
Toxicosis: The same as gestosis when used for pregnant woman. Also used in any severe acute disease, usually an infection, to describe a very ill looking patient (same as North American description "toxic-appearing.")
Trental (pentoxifylline): Used in the treatment of intermittent claudication associated with peripheral vascular disease.
Triampur: Combination diuretic containing triamterene and hydrochlorthiazide.
Umbilical hernia: We use the same term ... for some reason seems more common over there. Benign protrusion of the bellybutton caused by lax umbilical fibrous ring. Can look impressive, but is common, painless, easily reducible, and the majority resolve without intervention in a few years. Large, "elephant trunk" hernias are less likely to close on their own, but it's an easy day-surgery to fix. Does not need taping or any other "treatments".
Valerian: Dried rhizome and roots of valeriana officinalis, which is used as a sedative.
Vegeto-vascular syndrome: Symptoms thought to be associated with blood flow to internal organs, for example, frequent headaches or migraines in an older child or mottled skin in the infant.
Verospiron (spironolactone): Diuretic, aldosterone antagonist.
Vertizine (meclozine): Used in the prevention and treatment of nausea, vomiting and vertigo associated with motion sickness.
Vicasol: Synthetic vitamin K.
Viferon: Anti-viral, immunomodulating medication containing interferon and vitamins.
Wassermann test: Also written as RW. Screening test for syphilis.
Wydase: see Hyalase








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}